
Real-World Data: Possible Applications, Challenges & Emerging Role within Regulatory Affairs.
By Matthew Coombes.
Clinical Trials. Missing The Bigger Picture?
Clinical trials are historically associated with extensive inclusion and exclusion criteria, to deliver results which reflect an acceptable level of validity. Inclusion criteria typically focusses on distinct clinical and demographic features related to the nature of the research question being examined. On the other hand, exclusion criteria are applied to remove potential study participants who exhibit additional characteristics such as comorbidities, which may introduce bias (Patino and Ferreira, 2018).
Given the time and effort required to prepare for an interaction with FDA, it is crucial that the Applicant navigate the available options carefully in order to obtain as much value as possible from any one procedure. This paper will discuss the scope and procedure for each meeting type, based on FDA’s December 2017 Draft Guidance: Formal Meetings Between the FDA and Sponsors or Applicants of PDUFA Products1, as well as providing Scendea’s recommendations on strategy, timing, and meeting preparation, based on the first-hand in depth experience of our team of regulatory experts.
However, the use of clinical trial data in isolation for pharmaceutical development has been criticised for failing to provide results which are representative of the high degree of variability observed within the context of populations at large (Khosla et al., 2018). The stringent eligibility criteria used in clinical trials therefore simultaneously prevents the enrollment of a significant proportion of individuals from within the disease subpopulation of interest.
Evidence gaps have subsequently been identified, relating to variations in lifestyle factors and disease progression, both of which influence patient responses to therapeutics. Current predictions indicate a continued global trend of ‘population ageing’ due to improvements in healthcare and living standards (van der Cammen and Crome, 2018). These future demographic changes are expected to result in a greater number of individuals being prescribed multiple medications due to age-related conditions. This phenomenon may be responsible for causing an increased prevalence of adverse effects, a consequence of drug-drug interactions (Angamo et al., 2016; Cahir et al., 2017).
Clinical trials for therapies targeting conditions associated with old age such as cardiovascular diseases, typically have limited inclusion of older patients, due to a high incidence of individuals taking concomitant medications (Shenoy and Harugeri, 2015). The homogeneity among patient samples included within clinical studies therefore fails to capture accurate safety profiles, and may be responsible for causing avoidable morbidity within the elderly population.
Incidentally, these patients make up the vast bulk of pharmaceutical consumers. Furthermore, the ongoing coronavirus pandemic has led to significant disruption of clinical trials for other diseases, a consequence of funding withdrawals and social movement restrictions (TranspariMED, 2020). Subsequently, there is an increasing demand for including patient data in regulatory submissions collected from outside of the confines of the clinical trial environment (Baumfeld Andre et al., 2019).
Real-World Data (RWD)?
In contrast to clinical trial studies, Real-World Data (RWD) refers to patient health status information obtained from various sources, which can include Electronic Health Records (EHRs) from healthcare settings and personal wearable devices. Examples of RWD are presented in Figure 1. Large Real-world databases for healthcare related information exist, although these differ with respect to quality and therefore applicability for regulatory use Figure 2. Notably in the UK, the Clinical Practice Research Datalink (CPRD) has established itself as an interface between research sponsors and general practitioners (GPs), offering datasets for observational studies, with de-identified longitudinal data covering 53 million NHS patients with 20 years of follow up for 25% of individuals (CPRD, 2020).
Figure 1: Sources of RWD
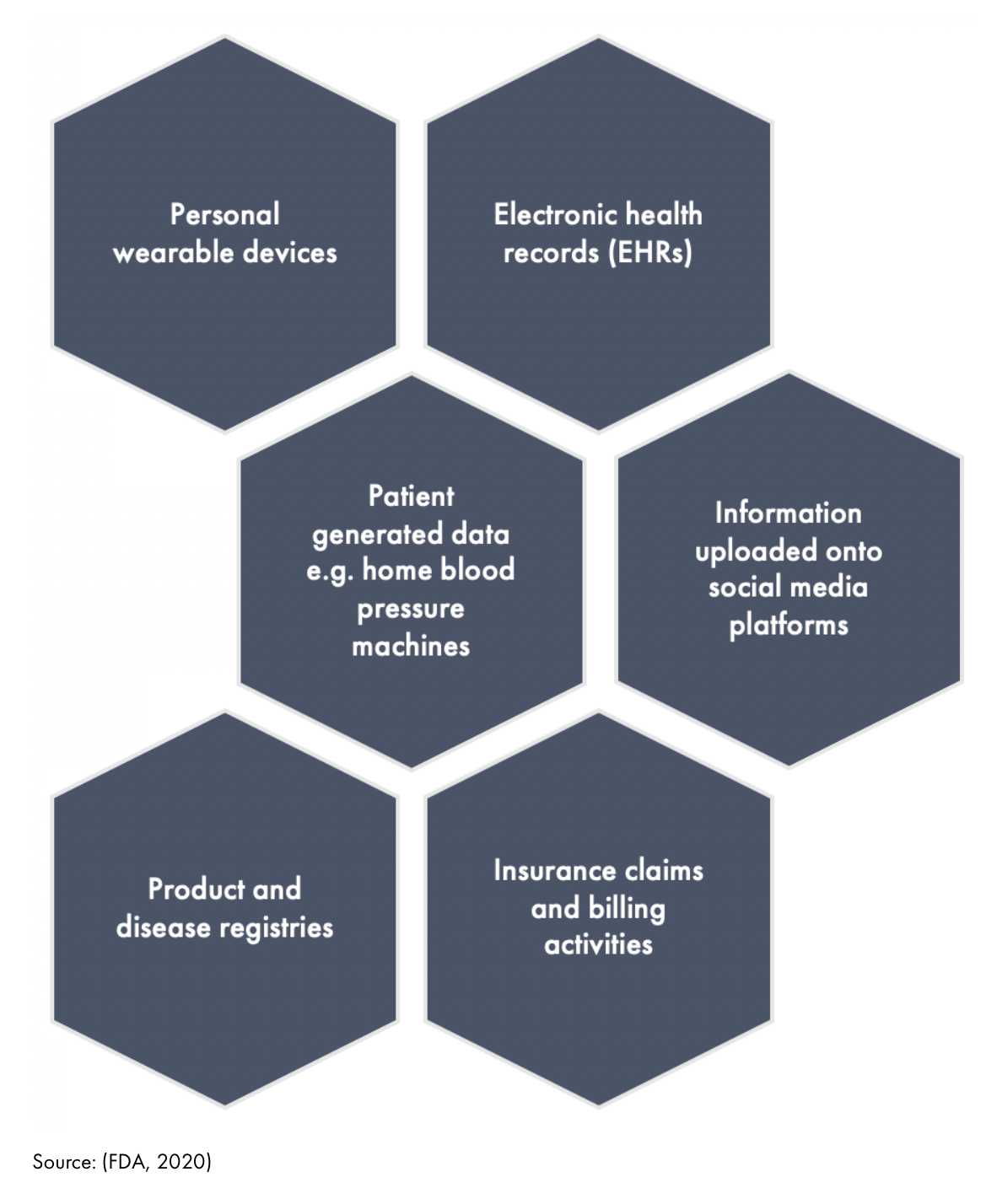
Figure 2: National Real-World databases

Applications of RWD.
Pre-Marketing.
The high availability of RWD and its analysis to provide Real-World Evidence (RWE) has been indicated as a possible mechanism of shortening timeframes required for clinical studies, and therefore allowing cost reductions in pharmaceutical development. Regulatory bodies have already indicated RWE is suitable for inclusion within submitted documentation for products. For example, Amgen has been granted approval for a cancer therapy based on submission of phase 2 study results combined with RWE (Xu, 2019). On the other hand, access to large amounts of patient data can enable trial investigators to identify patient groups with greatest possible benefits and risks prior to initiating clinical trial programmes, and thereby further customise marketing approvals.
Post-Marketing.
RWE may provide a powerful tool in enabling analysis of safety profiles after a product has received regulatory approval and entered the marketplace. This been shown in the case of a shingles vaccine where clinical trial data was lacking for long-term effectiveness in individuals aged 50-59 (FDA, 2020).
An observational study examining RWE collected from patients receiving the vaccine was undertaken by the sponsor, providing sufficient evidence for granting an update of the approved label to include long-term efficacy.
In addition, concerns were raised over a possible increased risk of serious cardiovascular events occurring in children and young adults receiving FDA approved drugs designed for managing the symptoms of Attention Deficit-Hyperactivity Disorder (ADHD). Undertaking clinical trials to examine the incidence of serious cardiovascular events in this context would raise significant technical challenges, due to a low prevalence of these events in this demographic group. Subsequently, any studies would require unfeasibly large numbers of patients for determining potential negative cardiovascular effects. In lieu of a traditional clinical trial, EHRs obtained from 4 health plans were analysed by researchers, amounting to over 1 million patients, indicating negligible increases in the risk of serious cardiovascular events (FDA, 2020).
RWE may be used to aid the expansion of indications for previously approved therapeutics (The Cancer Letter, 2019). For example, a supplemental New Drug Application (sNDA) composed of RWE obtained from EHRs, insurance claims and Pfizer’s global safety database was approved by the FDA to expand the use of Ibrance (Palbociclib) to include male breast cancer patients (Pharmaphorum, 2020). The potential uses of RWD are summarised in Figure 3.
Figure 3: Potential Uses of RWD

Real-World Data From a Regulatory Perspective – Applications For US & UK Marketed Products.
On December 13th 2016, the passing of the 21st Century Cures Act (Cures Act) in the US was designed to reduce the time required for the development of pharmaceuticals and allow patients faster access to novel products (Amgen, 2020). This Act includes a requirement for the US Food and Drug Administration (FDA) to develop appropriate information for relevant stakeholders to enable them to incorporate RWD within regulatory submissions. Specifically, the Cures Act dictates the need for guidance for RWD within the context of documents relating to post-approval safety and indication expansion. In 2019, the FDA published a draft document outlining the use of RWD for investigational new drug (IND), biologics license application (BLAs) and new drug application (NDAs) submissions. The guidance indicates applications using RWD will not be reviewed if the data included is not specific to a single product, or if the purpose of the application is not related to supporting decisions regarding safety or efficacy (FDA, 2019). In addition, the strength of RWD in regulatory submissions will be viewed by the FDA in relation to its relevance and quality control, with no specific data type receiving endorsement.
In contrast in the UK, RWD is acceptable for use in UK regulatory submissions, however no specific guidance is available from the Medicines and Healthcare products Regulatory Authority (MHRA) (ABPI, 2011). Sponsors wishing to undertake studies to collect RWD must do so in accordance with existing laws which indicate the need to maintain patient rights, dignity, and well-being. Studies intending to use RWD must meet several key criteria outlined in the Medicines for Human Use (clinical trials) Regulations 2004 (amended 2006). These criteria include medicines being prescribed in the usual manner and in relation to the approved marketing authorisation, a lack of randomisation of study participants, and the use of epidemiological methods for data analysis. Investigations meeting these requirements are not obliged to apply for a Clinical Trials Authorisation (CTA), and are categorised as non-interventional.
Challenges & Future Outlook.
Although RWD may offer significant benefits for the pharmaceutical industry, its use is currently restricted by several key barriers (Cave et al., 2019). Despite being highly abundant, concerns exist as to the quality of RWD, due to collection typically occurring within clinical care delivery settings. Patient records taken in this context are at greater risk of systematic and random error than in clinical trials, especially where patients are given full responsibility for self-reporting medical information. In addition, as RWD has not played a major role in product development, a lack of familiarity with its use among research teams is a potential issue, exacerbated by a limited number of suitable analytical tools for all possible RWD sources. Researchers have indicated mistrust of using RWD to conduct observational studies, highlighting such data may lack reproducibility. The historic tendency for regulatory documents to be solely based on clinical trial data means existing guidance surrounding the use of RWD in both the US and UK lacks clarity. However, both the FDA and MHRA have acknowledged the increasing desire of relevant stakeholders to take advantage of RWD, and expect to provide formalised guidance in 2021 (PharmaTimes, 2020; Gov UK, 2020).
Although RWD is available worldwide in the form of national databases, the bulk of these are restricted to several developed countries including Japan, the US, and the UK, meaning that fragmentation across geographical boundaries is a significant problem (Mckinsey and Company, 2018). In addition, the accessibility of information contained within healthcare databases varies significantly. Whilst the UK CPRD database is open for industry use through data purchase agreements, access to other databases such as the German WidO system are associated with lengthy waiting times and a need for interaction with academics. Notably, concerns over privacy has been highlighted as a factor in restricting industry access to these large datasets, and their use within regulatory submissions. In order to allow greater implementation of RWD within pharmaceutical development, it is apparent there is a pressing need for favourable govermental policies and incentives.
In conclusion, industry analysts have predicted stronger collaborations will be forged between primary healthcare systems and companies in the pharmaceutical industry wishing to obtain RWD.
These partnerships may include the development of more robust protocols for RWD use in observational studies, such as setting minimum requirements for the accuracy of measurements, which in turn may tighten feedback loops and improve clinical outcomes. Additional actions may involve the development of tools to enable integration of RWD from multiple sources to determine meaningful patterns for evaluating clinical performance, whilst continuing to maintain patient privacy and data security.
References.
ABPI (2011).
Amgen (2020).
Angamo, M., Chalmers (nee Stafford), L., Curtain, C., and Bereznicki, L. (2016). Adverse-Drug-Reaction-Related Hospitalisations in Developed and Developing Countries: A Review of Prevalence and Contributing Factors. Drug Safety 39.
Baumfeld Andre, E., Reynolds, R., Caubel, P., Azoulay, L., and Dreyer, N.A. (2019). Trial designs using real-world data: The changing landscape of the regulatory approval process. Pharmacoepidemiol Drug Saf.
Cahir, C., Curran, C., Byrne, C., Walsh, C., Hickey, A., Williams, D.J., and Bennett, K. (2017). Adverse Drug reactions in an Ageing PopulaTion (ADAPT) study protocol: a cross-sectional and prospective cohort study of hospital admissions related to adverse drug reactions in older patients. BMJ Open 7, e017322–e017322.
van der Cammen, T.J.M., and Crome, P. (2018). Persistent exclusion of older people from clinical trials of cardiovascular and antithrombotic medicinal products. European Geriatric Medicine 9, 413–414.
Cave, A., Kurz, X., and Arlett, P. (2019). Real-World Data for Regulatory Decision Making: Challenges and Possible Solutions for Europe. Clin Pharmacol Ther 106, 36–39.
CPRD (2020). Observational research.
FDA (2019). Submitting Documents Using Real-World Data and Real-World Evidence to FDA for Drugs and Biologics Guidance for Industry.
FDA (2020). Real World Evidence - From Safety to a Potential Tool for Advancing Innovative Ways to Develop New Medical Therapies.
Gov UK (2020). Medicines and Healthcare products Regulatory Agency Business Plan 2020 to 2021.
Khosla, S., White, R., Medina, J., Ouwens, M., Emmas, C., Koder, T., Male, G., and Leonard, S. (2018). Real world evidence (RWE) - a disruptive innovation or the quiet evolution of medical evidence generation? F1000Res 7, 111–111.
Mckinsey and Company , 2018. Real-world evidence: From activity to impact in healthcare decision making. [Online]
Available at: https://www.mckinsey.com/industries/pharmaceuticals-and-medical-products/our-insights/real-world-evidence-from-activity-to-impact-in-healthcare-decision-making [Accessed 10 February 2021].
Patino, C.M., and Ferreira, J.C. (2018). Inclusion and exclusion criteria in research studies: definitions and why they matter. J Bras Pneumol 44, 84–84.
Pharmaphorum (2020). The future of real world evidence.
PharmaTimes (2020). Six 2020 predictions for real-world evidence.
Shenoy, P., and Harugeri, A. (2015). Elderly patients’ participation in clinical trials. Perspect Clin Res 6, 184–189.
The Cancer Letter (2019). How real world evidence was used to support approval of Ibrance for male breast cancer.
Xu; Xuanyan (2019).